Diagnosis[edit]
Typical tests performed
| System | Tests |
|---|
| Kidney | Microscopic urinalysis, protein in the urine, BUN and/or creatinine |
| Endocrine | Serum sodium, potassium, calcium, TSH |
| Metabolic | Fasting blood glucose, HDL, LDL, and total cholesterol, triglycerides |
| Other | Hematocrit, electrocardiogram, and chest radiograph |
| Sources: Harrison's principles of internal medicine[57] others[58][59][60][61][62] |
Hypertension is diagnosed on the basis of a persistently high resting blood pressure. Traditionally, the
National Institute of Clinical Excellencerecommends three separate resting sphygmomanometer measurements at monthly intervals.
[63][64] The
American Heart Associationrecommends at least three resting measurements on at least two separate health care visits.
[65] Ambulatory blood pressure monitoring over 12 to 24 hours is the most accurate method to confirm the diagnosis.
[66]
An exception to this is those with very high blood pressure readings especially when there is poor
organ function.
[64] Initial assessment of the hypertensive people should include a complete
history and
physical examination. With the availability of 24-hour
ambulatory blood pressure monitors and
home blood pressure machines, the importance of not wrongly diagnosing those who have
white coat hypertension has led to a change in protocols. In the United Kingdom, current best practice is to follow up a single raised clinic reading with ambulatory measurement, or less ideally with home blood pressure monitoring over the course of 7 days.
[64] The United States Preventative Services Task Force also recommends getting measurements outside of the healthcare environment.
[67] Pseudohypertension in the elderly or noncompressibility artery syndrome may also require consideration. This condition is believed to be due to calcification of the arteries resulting in abnormally high blood pressure readings with a blood pressure cuff while intra arterial measurements of blood pressure are normal.
[68] Orthostatic hypertension is when blood pressure increases upon standing.
[69]
Once the diagnosis of hypertension has been made, healthcare providers should attempt to identify the underlying cause based on risk factors and other symptoms, if present.
Secondary hypertension is more common in preadolescent children, with most cases caused by
kidney disease. Primary or
essential hypertension is more common in adolescents and has multiple risk factors, including obesity and a family history of hypertension.
[70] Laboratory tests can also be performed to identify possible causes of secondary hypertension, and to determine whether hypertension has caused damage to the
heart,
eyes, and
kidneys. Additional tests for
diabetes and
high cholesterol levels are usually performed because these conditions are additional risk factors for the development of
heart disease and may require treatment.
[6]
Serum
creatinine is measured to assess for the presence of kidney disease, which can be either the cause or the result of hypertension. Serum creatinine alone may overestimate
glomerular filtration rate and recent guidelines advocate the use of predictive equations such as the
Modification of Diet in Renal Disease (MDRD) formula to estimate glomerular filtration rate (eGFR).
[71] eGFR can also provide a baseline measurement of kidney function that can be used to monitor for side effects of certain antihypertensive drugs on kidney function. Additionally, testing of urine samples for
protein is used as a secondary indicator of kidney disease.
Electrocardiogram (EKG/ECG) testing is done to check for evidence that the heart is under strain from high blood pressure. It may also show whether there is thickening of the heart muscle (
left ventricular hypertrophy) or whether the heart has experienced a prior minor disturbance such as a silent heart attack. A
chest X-ray or an
echocardiogram may also be performed to look for signs of heart enlargement or damage to the heart.
[18]
In people aged 18 years or older hypertension is defined as a systolic and/or a diastolic blood pressure measurement consistently higher than an accepted normal value (currently 139 mmHg systolic, 89 mmHg diastolic: see table – Classification (JNC7)). Lower thresholds are used (135 mmHg systolic or 85 mmHg diastolic) if measurements are derived from 24-hour ambulatory or home monitoring.
[64] Recent international hypertension guidelines have also created categories below the hypertensive range to indicate a continuum of risk with higher blood pressures in the normal range. JNC7 (2003)
[71] uses the term prehypertension for blood pressure in the range 120–139 mmHg systolic and/or 80–89 mmHg diastolic, while ESH-ESC Guidelines (2007)
[72] and BHS IV (2004)
[73] use optimal, normal and high normal categories to subdivide pressures below 140 mmHg systolic and 90 mmHg diastolic. Hypertension is also sub-classified: JNC7 distinguishes hypertension stage I, hypertension stage II, and isolated systolic hypertension. Isolated systolic hypertension refers to elevated systolic pressure with normal diastolic pressure and is common in the elderly.
[71] The ESH-ESC Guidelines (2007)
[72] and BHS IV (2004)
[73]additionally define a third stage (stage III hypertension) for people with systolic blood pressure exceeding 179 mmHg or a diastolic pressure over 109 mmHg. Hypertension is classified as "resistant" if
medications do not reduce blood pressure to normal levels.
[71]
Children[edit]
Hypertension occurs in around 0.2 to 3% of newborns; however, blood pressure is not measured routinely in healthy newborns.
[28] Hypertension is more common in high risk newborns. A variety of factors, such as
gestational age, postconceptional age and
birth weight needs to be taken into account when deciding if a blood pressure is normal in a newborn.
[28]
Hypertension defined as elevated blood pressure over several visits affects 1% to 5% of children and adolescents and is associated with long term risks of ill-health.
[74] Blood pressure rises with age in childhood and, in children, hypertension is defined as an average systolic or diastolic blood pressure on three or more occasions equal or higher than the 95th percentile appropriate for the sex, age and height of the child. High blood pressure must be confirmed on repeated visits however before characterizing a child as having hypertension.
[74] Prehypertension in children has been defined as average systolic or diastolic blood pressure that is greater than or equal to the 90th percentile, but less than the 95th percentile.
[74] In adolescents, it has been proposed that hypertension and pre-hypertension are diagnosed and classified using the same criteria as in adults.
[74]
Prevention[edit]
Much of the disease burden of high blood pressure is experienced by people who are not labeled as hypertensive.
[73] Consequently, population strategies are required to reduce the consequences of high blood pressure and reduce the need for antihypertensive drug therapy. Lifestyle changes are recommended to lower blood pressure, before starting drug therapy. The 2004 British Hypertension Society guidelines
[73] proposed lifestyle changes consistent with those outlined by the US National High BP Education Program in 2002
[80] for the primary prevention of hypertension:
- maintain normal body weight for adults (e.g. body mass index 20–25 kg/m2)
- reduce dietary sodium intake to <100 mmol/ day (<6 g of sodium chloride or <2.4 g of sodium per day)
- engage in regular aerobic physical activity such as brisk walking (≥30 min per day, most days of the week)
- limit alcohol consumption to no more than 3 units/day in men and no more than 2 units/day in women
- consume a diet rich in fruit and vegetables (e.g. at least five portions per day);
Effective lifestyle modification may lower blood pressure as much as an individual antihypertensive drug. Combinations of two or more lifestyle modifications can achieve even better results.
[73] There is considerable evidence that reducing dietary salt intake lowers blood pressure, but whether this translates into a reduction in mortality and cardiovascular disease remains uncertain.
[81] Estimated sodium intake ≥6g/day and <3g/day are both associated with high risk of death and/or major cardiovascular disease, but the association between high sodium intake and adverse outcomes is only observed in people with hypertension.
[82] Consequently, in the absence of results from randomized controlled trials, the wisdom of reducing levels of dietary salt intake below 3g/day has been questioned.
[81]
Management[edit]
Target blood pressure[edit]
Various expert groups have produced guidelines regarding how low the blood pressure target should be when a person is treated for hypertension. These groups recommend a target below the range 140–160 / 90–100 mmHg for the general population.
[8][84][85][86][87] Controversy exists regarding the appropriate targets for certain subgroups, including the elderly, people with diabetes and people with kidney disease.
[88]
Many expert groups recommend a slightly higher target of 150/90 mmHg for those over 80 years of age.
[84][85][86] One expert group, the JNC-8, recommends the target of 150/90 mmHg for those over 60 years of age,
[8] but some experts within this group disagree with this recommendation.
[89] Some expert groups have also recommended slightly lower targets in those with diabetes
[84] or chronic kidney disease with proteinuria,
[90] but others recommend the same target as for the general population.
[8][88] The issue of what is the best target and whether targets should differ for high risk individuals is unresolved,
[91] but current best evidence supports more intensive blood pressure lowering than advocated in some guidelines.
[92]
Lifestyle modifications[edit]
The first line of treatment for hypertension is lifestyle changes, including dietary changes, physical exercise, and weight loss. Though these have all been recommended in scientific advisories,
[93] a
Cochrane systematic review found no evidence for effects of weight loss diets on death or long-term complications and adverse events in persons with hypertension.
[94] The review did find a decrease in blood pressure.
[94] Their potential effectiveness is similar to and at times exceeds a single medication.
[7] If hypertension is high enough to justify immediate use of medications, lifestyle changes are still recommended in conjunction with medication.
Dietary changes shown to reduce blood pressure include diets with low sodium,
[95][96][needs update][97] the
DASH diet,
[98] and vegetarian diets.
[99] While potassium supplementation is useful it is unclear if a high dietary potassium intake is beneficial.
[100][101]
Medications[edit]
Resistant hypertension[edit]
Resistant hypertension is defined as hypertension that remains above goal blood pressure in spite of using, at once, three antihypertensive medications belonging to different drug classes. Low adherence to treatment is an important cause of resistant hypertension.
[106] Resistant hypertension may also represent the result of chronic high activity of the
autonomic nervous system; this concept is known as "neurogenic hypertension".
[107]
Epidemiology[edit]
As of 2014, approximately one billion adults or ~22% of the population of the world have hypertension.
[109] It is slightly more frequent in men,
[109] in those of low
socioeconomic status,
[6] and
prevalence increases with age.
[6] It is common in high, medium and low income countries.
[109][110] The prevalence of raised blood pressure is highest in Africa, (30% for both sexes) and lowest in the WHO Region of the Americas (18% for both sexes). Rates also vary markedly within WHO regions with rates as low as 3.4% (men) and 6.8% (women) in rural India and as high as 68.9% (men) and 72.5% (women) in Poland.
[111] In Europe hypertension occurs in about 30-45% of people as of 2013.
[7] In 1995 it was estimated that 43 million people (24% of the populations) in the United States had hypertension or were taking antihypertensive medication.
[112] By 2004 this had increased to 29%
[113][114] and further to 34% (76 million US adults) by 2006. African American adults in the United States have among the highest rates of hypertension in the world at 44%.
[115] It is also more common in
Filipino Americans and less common in US
whites and
Mexican Americans.
[6][116]
Children[edit]
Rates of high blood pressure in children and adolescents have increased in the last 20 years in the United States.
[117] Childhood hypertension, particularly in pre-adolescents, is more often secondary to an underlying disorder than in adults. Kidney disease is the most common secondary cause of hypertension in children and adolescents. Nevertheless, primary or essential hypertension accounts for most cases.
[118]
Outcomes[edit]
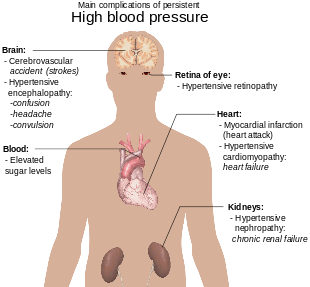
Diagram illustrating the main complications of persistent high blood pressure
History[edit]
Image of veins from Harvey's
Exercitatio Anatomica de Motu Cordis et Sanguinis in Animalibus
Measurement[edit]
Modern understanding of the cardiovascular system began with the work of physician
William Harvey (1578–1657), who described the circulation of blood in his book "
De motu cordis". The English clergyman
Stephen Hales made the first published measurement of blood pressure in 1733.
[122][123] However hypertension as a clinical entity came into its own in 1896 with the invention of the cuff-based
sphygmomanometer by
Scipione Riva-Rocci in 1896.
[124] This allowed easy measurement of systolic pressure in the clinic. In 1905,
Nikolai Korotkoff improved the technique by describing the
Korotkoff sounds that are heard when the artery is ausculated with a stethoscope while the sphygmomanometer cuff is deflated.
[123]This permitted systolic and diastolic pressure to be measured.
Identification[edit]
The symptoms similar to symptoms of patients with hypertensive crisis are discussed in medieval Persian medical texts in the chapter of "fullness disease".
[125] The symptoms include headache, heaviness in the head, sluggish movements, general redness and warm to touch feel of the body, prominent, distended and tense vessels, fullness of the pulse, distension of the skin, coloured and dense urine, loss of appetite, weak eyesight, impairment of thinking, yawning, drowsiness, vascular rupture, and hemorrhagic stroke.
[126]Fullness disease was presumed to be due to an excessive amount of blood within the blood vessels.
Treatment[edit]
Historically the treatment for what was called the "hard pulse disease" consisted in reducing the quantity of blood by
bloodletting or the application of
leeches.
[122] This was advocated by The
Yellow Emperor of China,
Cornelius Celsus,
Galen, and
Hippocrates.
[122] The therapeutic approach for the treatment of hard pulse disease included changes in lifestyle (staying away from anger and sexual intercourse) and dietary program for patients (avoiding the consumption of wine, meat, and pastries, reducing the volume of food in a meal, maintaining a low-energy diet and the dietary usage of spinach and vinegar).
In the 19th and 20th centuries, before effective pharmacological treatment for hypertension became possible, three treatment modalities were used, all with numerous side-effects: strict sodium restriction (for example the rice diet
[122]),
sympathectomy (surgical ablation of parts of the
sympathetic nervous system), and pyrogen therapy (injection of substances that caused a fever, indirectly reducing blood pressure).
[122][128]
The first chemical for hypertension,
sodium thiocyanate, was used in 1900 but had many side effects and was unpopular.
[122] Several other agents were developed after the
Second World War, the most popular and reasonably effective of which were
tetramethylammonium chloride,
hexamethonium,
hydralazine and
reserpine (derived from the medicinal plant
Rauwolfia serpentina). None of these were well tolerated.
[129][130] A major breakthrough was achieved with the discovery of the first well-tolerated orally available agents. The first was
chlorothiazide, the first
thiazide diuretic and developed from the antibiotic
sulfanilamide, which became available in 1958.
[122][131] Subsequently
beta blockers,
calcium channel blockers,
angiotensin converting enzyme (ACE) inhibitors,
angiotensin receptor blockers and
renin inhibitors were developed as antihypertensive agents.
[128]
Society and culture[edit]
Awareness[edit]

Graph showing, prevalence of awareness, treatment and control of hypertension compared between the four studies of
NHANES[113]
The World Health Organization has identified hypertension, or high blood pressure, as the leading cause of
cardiovascular mortality.
[132]The World Hypertension League (
WHL), an umbrella organization of 85 national hypertension societies and leagues, recognized that more than 50% of the hypertensive population worldwide are unaware of their condition.
[132] To address this problem, the WHL initiated a global awareness campaign on hypertension in 2005 and dedicated May 17 of each year as
World Hypertension Day (
WHD). Over the past three years, more national societies have been engaging in WHD and have been innovative in their activities to get the message to the public. In 2007, there was record participation from 47 member countries of the WHL. During the week of WHD, all these countries – in partnership with their local governments, professional societies, nongovernmental organizations and private industries – promoted hypertension awareness among the public through several
media and public rallies. Using
mass media such as Internet and television, the message reached more than 250 million people. As the momentum picks up year after year, the WHL is confident that almost all the estimated 1.5 billion people affected by elevated blood pressure can be reached.
[133]
Economics[edit]
High blood pressure is the most common chronic medical problem prompting visits to primary health care providers in USA. The American Heart Association estimated the direct and indirect costs of high blood pressure in 2010 as $76.6 billion.
[115] In the US 80% of people with hypertension are aware of their condition, 71% take some antihypertensive medication, but only 48% of people aware that they have hypertension adequately control it.
[115] Adequate management of hypertension can be hampered by inadequacies in the diagnosis, treatment, and/or control of high blood pressure.
[134] Health care providers face many obstacles to achieving blood pressure control, including resistance to taking multiple medications to reach blood pressure goals. People also face the challenges of adhering to medicine schedules and making lifestyle changes. Nonetheless, the achievement of blood pressure goals is possible, and most importantly, lowering blood pressure significantly reduces the risk of death due to heart disease and stroke, the development of other debilitating conditions, and the cost associated with advanced medical care.
[135][136]
















_Venenbild.jpg)









